Cortisol is the most consequential hormone in your brain’s operating system, and the most misread. Most people encounter the word in the context of stress, burnout, or weight gain, which tells a fraction of the story and misses the part that actually matters. Cortisol is not the enemy. It is a precision instrument that your brain uses to regulate alertness, immunity, metabolism, memory, and inflammatory response across every hour of the day. The problem is not that you have cortisol. The problem is what happens when the system that governs it stops calibrating accurately.
In my practice, I work with individuals whose cortisol dysregulation is driving outcomes they’ve attributed to everything except their neurobiology: the decision paralysis, the emotional brittleness, the cognitive fog at 2 p.m., the wired-but-exhausted sensation that no amount of sleep resolves. Once we identify the hormonal architecture underneath these patterns, the intervention becomes precise. Not supplementation. Not breathwork. Neural rewiring of the feedback mechanisms that govern cortisol output in the first place.
This page brings together 23 articles from the MindLAB library examining cortisol from every meaningful angle: its circadian architecture, its role in the HPA axis feedback loop, what chronic elevation does to hippocampal tissue, how it interacts with cognitive performance, and the methodology I use to regulate it at the neurological level.
Cortisol Is Not a Stress Hormone: It Is a Regulatory Hormone
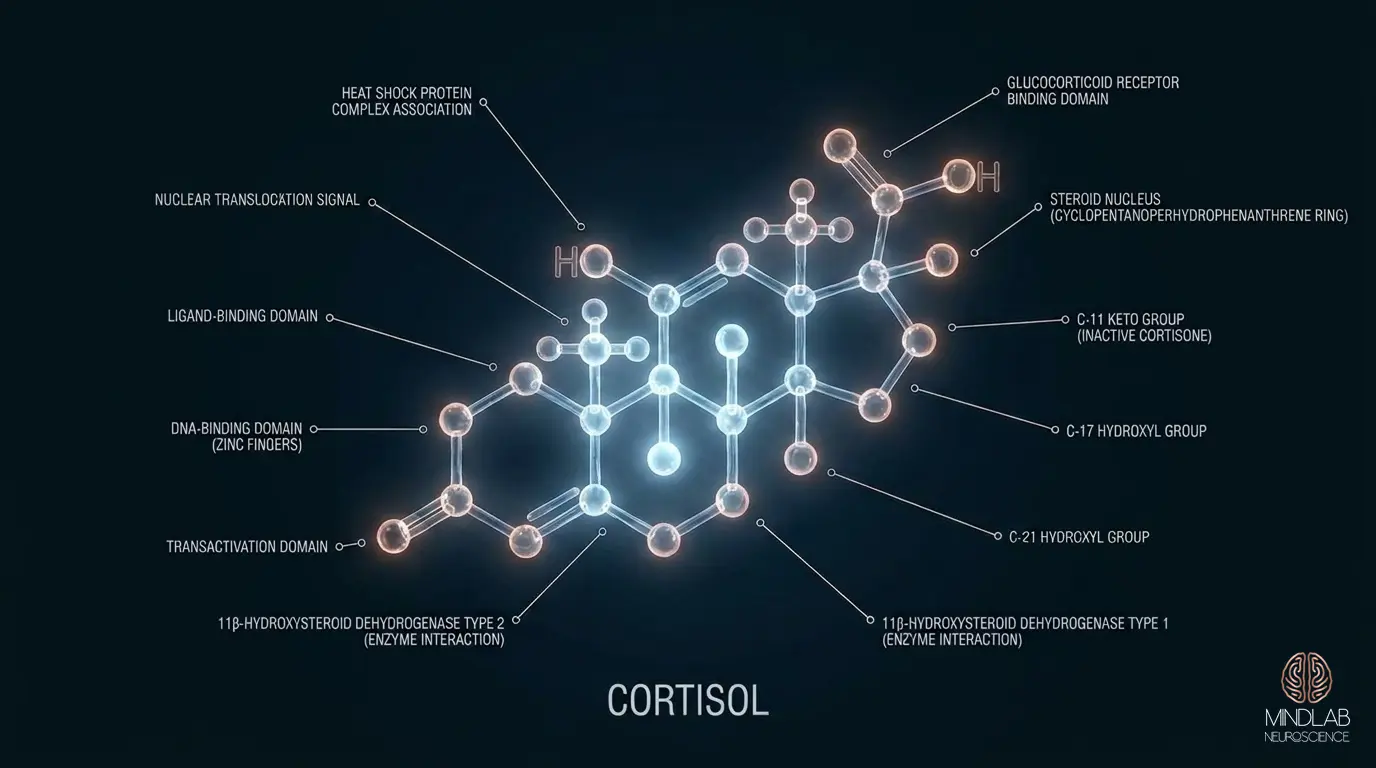
The single most persistent misconception about cortisol is that its purpose is to respond to stress. That framing is accurate but incomplete, and the incompleteness is what leads people to pursue interventions that miss the mechanism entirely. Cortisol is produced by the adrenal cortex and follows a precise daily rhythm governed by your hypothalamic-suprachiasmatic nucleus circuit: the brain’s master clock. On a healthy cortisol curve, levels peak approximately 30 to 45 minutes after waking, remain elevated through mid-morning to support alertness and metabolic activation, decline steadily through the afternoon, and reach their nadir around midnight to permit restorative sleep architecture.
This rhythm exists independently of whether you experience anything stressful on a given day. Your cortisol is rising before you open your eyes, driven by light-sensitive neural signals from the retina to the hypothalamus. It is managing your immune surveillance, regulating blood glucose, and priming the prefrontal cortex for executive function, all before your first decision of the day. Stress-reactive cortisol spikes are a secondary function layered on top of a primary regulatory architecture. Treating cortisol as a stress variable and ignoring its baseline circadian role is like diagnosing a broken thermostat by only measuring the temperature when the front door opens.
When I encounter a client whose cortisol output is dysregulated, my first assessment is not “what stressors are they experiencing?” It is: what has disrupted the circadian driver? Sleep fragmentation, artificial light exposure after dark, irregular eating patterns, and chronic sympathetic activation all erode the precision of the cortisol curve before any acute stressor enters the picture. The stressor reveals the dysregulation; it rarely creates it from scratch.
The Cortisol Awakening Response: Your Brain’s Daily Calibration Signal
One of the most diagnostically useful cortisol phenomena, and one of the least discussed outside specialist literature, is the cortisol awakening response (CAR). In the 20 to 30 minutes immediately following waking, a healthy brain produces a sharp surge in cortisol that can reach 50 to 160 percent above pre-waking baseline. This is not incidental. It is a deliberate neural preparation sequence.
The CAR appears to serve three coordinated functions: it activates the immune system’s morning surveillance sweep, primes hippocampal memory consolidation systems for the demands of the coming day, and signals to peripheral organs, including the liver and immune tissue, that the circadian day has begun. Research published in Psychoneuroendocrinology has linked a robust CAR to superior working memory performance and more adaptive stress responses throughout the day. A blunted CAR, cortisol that barely moves after waking, is associated with burnout, hypothalamic-pituitary-adrenal (HPA) axis suppression, and increased inflammatory biomarkers.
In my practice, I consistently observe that clients who report “not being morning people” or requiring extended ramp-up time before cognitive performance stabilizes frequently show a flattened cortisol awakening response. Their brains are not failing to wake up. Their HPA axis has downregulated the morning surge, often as a protective response to sustained cortisol overactivation in preceding months. The brain has concluded, at the level of glucocorticoid receptor sensitivity, that high-amplitude cortisol is no longer safe to produce. This adaptive suppression then produces its own set of functional impairments, and the cycle continues.
The HPA Axis Feedback Loop: Where Regulation Breaks Down
Cortisol does not regulate itself. It is governed by a three-part feedback architecture called the hypothalamic-pituitary-adrenal (HPA) axis. The hypothalamus releases corticotropin-releasing hormone (CRH), which signals the pituitary to release adrenocorticotropic hormone (ACTH), which signals the adrenal glands to release cortisol. What makes this system intelligent is the negative feedback loop: cortisol itself binds to glucocorticoid receptors in the hippocampus and prefrontal cortex, signaling the hypothalamus to reduce CRH output. The system is designed to self-correct.
Chronic stress, chronic cortisol elevation, and chronic sleep insufficiency all degrade this feedback mechanism through a process called glucocorticoid receptor downregulation. When cortisol is chronically elevated, the hippocampus and prefrontal cortex reduce the density of glucocorticoid receptors as a protective measure, a breakdown in the same stress and nervous system regulation architecture that governs autonomic balance, essentially becoming less sensitive to the “turn off” signal. The hypothalamus, no longer receiving adequate negative feedback, continues driving CRH output. Cortisol stays elevated. Receptor sensitivity continues to decline. The feedback loop that was designed to be self-correcting becomes self-perpetuating.
This is not a metaphor. A landmark study by McEwen and colleagues at Rockefeller University quantified glucocorticoid receptor loss in the hippocampus following sustained cortisol exposure, establishing the structural basis for what clinicians observe behaviorally: an individual whose stress response system no longer turns off on its own. The brain is not being irrational. It has structurally adapted to an environment it perceived as chronically threatening, and that adaptation has a measurable neural substrate.
In my work, identifying where in this loop the breakdown is occurring (whether the problem is excessive cortisol production, receptor insensitivity, or a compromised negative feedback circuit) determines the entire direction of intervention. These are not interchangeable problems. They require categorically different approaches at the neural level.
Chronic Cortisol Elevation and Hippocampal Damage
The hippocampus is cortisol’s primary target organ in the brain, and it is also cortisol’s primary casualty when regulation fails. The hippocampus is densely populated with glucocorticoid receptors, more than virtually any other brain structure. This density serves the feedback function described above: the hippocampus monitors cortisol levels and helps calibrate the shutoff signal. But this density also makes hippocampal neurons exceptionally vulnerable to glucocorticoid toxicity when cortisol remains elevated for extended periods.
The research literature on cortisol-induced hippocampal atrophy is among the most replicated findings in behavioral neuroscience. Sapolsky’s foundational work with primate models demonstrated that sustained cortisol elevation produces measurable dendritic retraction in hippocampal neurons: the neurons physically shrink, reducing synaptic connectivity. Subsequent human neuroimaging studies have confirmed volumetric reductions in the hippocampus in individuals with major depression, post-traumatic stress, and chronic burnout and neural depletion, all conditions associated with HPA axis dysregulation and chronically elevated cortisol.
The functional consequences are significant and specific. The hippocampus governs episodic memory consolidation, spatial navigation, contextual fear learning, and, critically, the ability to distinguish between a genuine threat and a perceived one. When the hippocampus is compromised by chronic cortisol exposure, the brain loses precision in its threat-appraisal function. Everything begins to register as high-stakes. The individual experiences what they describe as disproportionate reactivity, an inability to “let things go,” and a cognitive system that cannot reliably distinguish signal from noise.
I want to be precise about what this means in practice: hippocampal damage from cortisol dysregulation is not a permanent sentence. Neuroplasticity research, including work from the Bhagya Nair lab at the Salk Institute, has demonstrated hippocampal volume recovery following effective intervention. The brain’s capacity to rebuild dendritic complexity in the hippocampus when cortisol regulation is restored is one of the most compelling arguments for addressing cortisol dysregulation at its neural source rather than managing its downstream behavioral symptoms.
Cortisol and Cognitive Performance: The Inverted-U That Most People Miss
There is a fundamental relationship between cortisol and cognitive performance that the popular understanding of “cortisol is bad” completely obscures. The relationship is not linear: it is an inverted U. Performance improves as cortisol rises from baseline, reaches a peak at moderate arousal levels, and then degrades sharply as cortisol continues to rise. This is the Yerkes-Dodson principle operating through cortisol as the hormonal mediator.
What this means in practice: the cortisol that rises in anticipation of a meaningful challenge, that sharpens focus before a high-stakes presentation, that heightens sensory acuity before a critical decision: that cortisol is not the problem. It is functioning exactly as designed. The problem begins when cortisol cannot return to baseline after the challenge passes, when the moderate activation that serves performance becomes the chronic elevation that impairs it.
In my practice, I work with executives who have spent years operating in the elevated half of the inverted-U curve, interpreting the cortisol-driven sharpness as their natural performance state. They have mistaken the activation for their identity. When the cortisol system eventually degrades, because no feedback loop can sustain chronic overactivation indefinitely, they experience the performance decline as evidence of personal failure rather than as a predictable physiological consequence. The intervention begins with that reframe: your brain did not fail you. It ran an unsustainable program at maximum load for too long, and it is now enforcing a correction.
Prefrontal cortex function is particularly sensitive to cortisol levels. At optimal levels, cortisol enhances prefrontal dopamine signaling, the same circuitry explored across brain health optimization and neuroprotection research, improving working memory, attention, and decision precision. At elevated levels, it suppresses prefrontal function via norepinephrine pathways, impairing the cognitive flexibility, error monitoring, and strategic thinking that high-performance individuals depend on most. The executives who describe “losing their edge” at mid-career are frequently describing the downstream cognitive consequences of HPA axis dysregulation, not the natural arc of aging.
Cortisol’s Immune and Metabolic Role: What Stays Hidden
The stress narrative about cortisol has obscured two domains where its dysregulation produces measurable harm that most people never connect to the source. The first is immune regulation. Cortisol is the body’s primary endogenous anti-inflammatory signal: in acute, time-limited doses, it suppresses inflammatory cytokine production and modulates immune activation appropriately. The immune system depends on this suppressive signal to prevent overreaction to routine environmental challenges.
When cortisol is chronically elevated, the immune system adapts by reducing glucocorticoid receptor sensitivity: the same receptor downregulation described in the HPA axis context. The result is a paradox: chronically elevated cortisol paradoxically produces chronic low-grade inflammation, because the immune cells that would normally respond to cortisol’s anti-inflammatory signal have lost their sensitivity to it. Research published in PNAS by Cohen and colleagues quantified this mechanism, demonstrating that individuals with blunted glucocorticoid receptor sensitivity following chronic stress showed elevated inflammatory markers despite having cortisol levels that should have suppressed them.
The metabolic consequences operate through a separate but parallel mechanism. Cortisol mobilizes glucose from liver stores and muscle tissue to fuel the fight-or-flight response. In acute scenarios, this is adaptive. In chronic elevation, it produces persistent hyperglycemia, accelerated visceral fat deposition, driven by cortisol receptors that are particularly dense in abdominal adipose tissue, and dysregulation of insulin sensitivity. The individuals in my practice who report unexplained weight gain concentrated in the midsection, persistent energy fluctuations, and carbohydrate cravings in the afternoon are frequently experiencing the metabolic signature of a cortisol system that never fully down-regulates.
Dr. Ceruto’s Cortisol Regulation Methodology
In 26 years of practice, I have not encountered a single client whose cortisol dysregulation was primarily a lifestyle problem. Reducing caffeine intake, practicing sleep hygiene, or adding morning sunlight exposure may shift the curve slightly at the margins, but they do not address the neural architecture driving the dysregulation. Cortisol is downstream of a regulatory system that is itself governed by neural patterns: patterns of threat appraisal, patterns of rumination, patterns of autonomic activation that the brain runs automatically, below the threshold of conscious decision-making.
My methodology for cortisol regulation begins at the level of the HPA axis feedback loop itself: specifically, at the threat-appraisal patterns in the prefrontal cortex and amygdala that are driving the cortisol output in the first place. Real-Time Neuroplasticity™ intervenes in the live moment when these patterns activate, not retrospectively through reflection or journaling. The distinction matters neurologically: a pattern that is interrupted and replaced in its actual firing state produces structural synaptic change. A pattern that is analyzed after the fact produces insight without neural reconfiguration.
The first phase of my cortisol-focused work is precise identification: which specific appraisal patterns are sustaining HPA axis activation? For some clients, it is a pattern of scanning for social threat: hypervigilance to interpersonal criticism that the amygdala has been trained to treat as existential. For others, it is a time-pressure schema that activates the threat response to any open slot on a calendar. For others still, it is the identity-threat pattern that interprets any ambiguity as evidence of inadequacy. Each of these patterns drives cortisol through a specific neural pathway, and each requires a specific intervention architecture.
The second phase targets the glucocorticoid receptor sensitivity that has been eroded by sustained exposure. This involves working directly with the hypothalamic regulation capacity, through real-time interoceptive awareness training, to begin restoring the brain’s ability to receive and act on the cortisol shutoff signal. This is not relaxation training. It is precision neural work designed to rebuild the feedback infrastructure that chronic cortisol elevation has degraded.
What I observe consistently in this work: within 8 to 12 weeks of sustained real-time intervention, clients report not that they experience fewer stressors, but that their cortisol response to identical stressors has changed. The spike is lower. The recovery is faster. The cognitive degradation that used to follow high-stress periods no longer materializes at the same intensity. This is not behavioral adaptation. It is the functional signature of a restored HPA axis feedback loop.
What the Research on Cortisol Gets Wrong, and What My Practice Has Shown
The research literature on cortisol is excellent on mechanism and often inadequate on intervention. The dominant clinical framework treats cortisol dysregulation as a secondary symptom: manage the primary condition (the anxiety, the depression, the burnout), and cortisol will normalize. In my experience, this gets the causal direction backwards in a meaningful percentage of cases.
For many of the individuals I work with, the dysregulation in mood, motivation, and cognitive performance IS the cortisol dysregulation. There is no separate “primary” condition beneath it. The pattern is not that cortisol is elevated because they are anxious: it is that the neural architecture that governs cortisol output has been miscalibrated, and the anxiety, the motivation loss, the cognitive brittleness are all downstream of that miscalibration. Address the neural driver, and the symptoms reorganize.
I also want to address what the literature misses about individual variation in cortisol reactivity. Baseline cortisol profiles vary significantly between individuals, and these variations are partially heritable through glucocorticoid receptor gene polymorphisms (specifically FKBP5 variants, which have been studied extensively in the context of stress reactivity and PTSD risk). A cortisol level that represents moderate activation in one individual may represent significant dysregulation in another. Population-level reference ranges for cortisol are not clinically meaningful guides for individual assessment. What matters is the pattern over time, the amplitude of the CAR, the rate of recovery from acute spikes, and the relationship between reported experience and hormonal output, all of which require longitudinal observation, not a single-point serum test.
The articles collected here approach cortisol from multiple directions: circadian, cognitive, relational, metabolic, and neural recalibration. They are not self-help protocols. They are explanatory frameworks designed to help you understand the biology driving your experience. If what you read resonates, and you are ready to work with the neural architecture rather than the surface behavior, I invite you to schedule a strategy call with Dr. Ceruto. That conversation begins the process of identifying exactly where in your cortisol regulatory system the intervention needs to occur.