The Brain Behind Imposter Syndrome: What’s Actually Happening in Your Neural Architecture
Imposter syndrome is not a personality quirk, a confidence problem, or a deficit in self-belief. It is a measurable neurological pattern: one that specific regions of the brain generate in response to a very particular kind of threat. Understanding what that threat is, and why your brain treats it as such, changes the entire conversation.
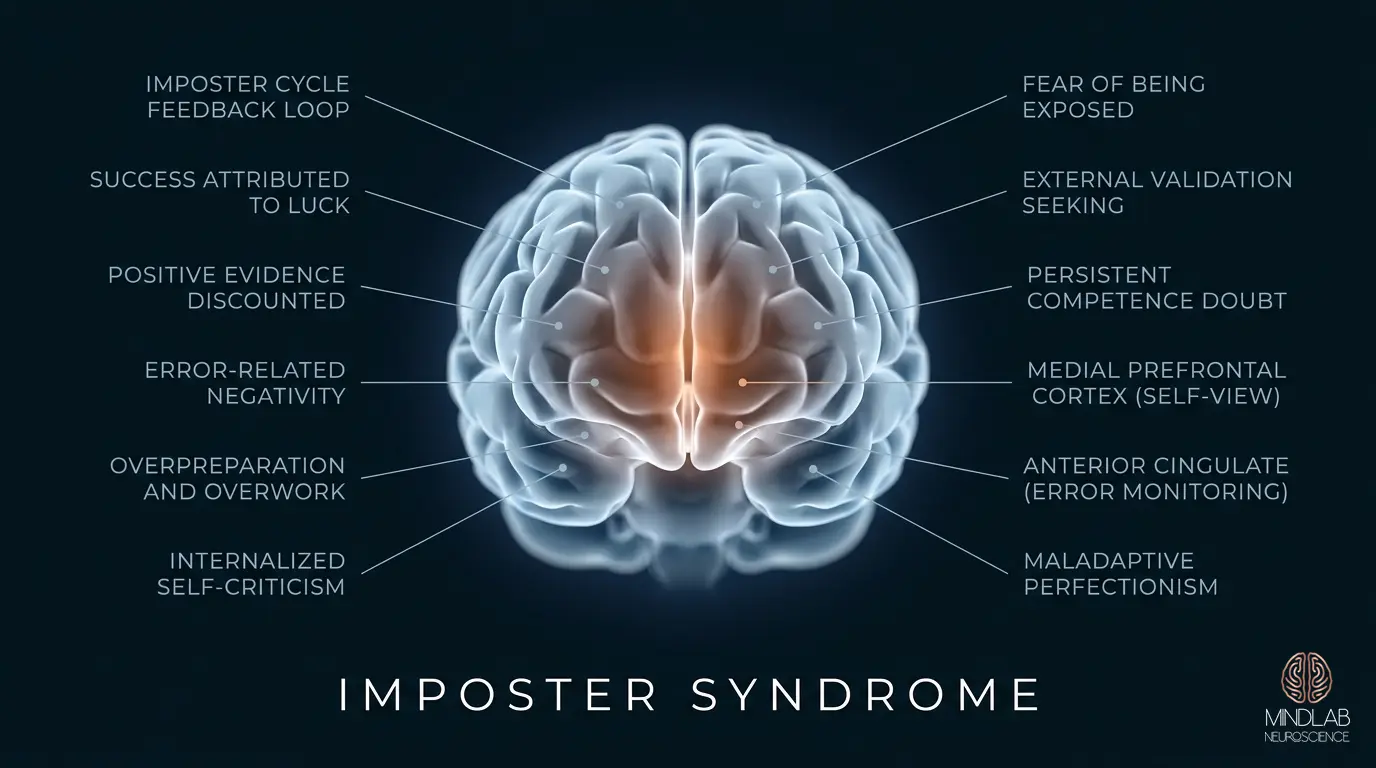
The experience most people describe involves a persistent, gnawing sense that their success has been unearned, that their knowledge is insufficient, and that at any moment, someone in authority is going to look past the performance and see the inadequacy underneath. This pattern sits at the intersection of self-awareness and interoceptive processing and the brain’s threat-detection architecture. What neuroscience has established is that this pattern is not irrational. It is a predictable output from a brain that has received confusing, contradictory signals about identity and competence, and responded with what it knows how to do best: generate vigilance.
The Anterior Cingulate Cortex and the Error-Detection Problem
At the center of imposter syndrome’s neural signature is the anterior cingulate cortex, a region positioned along the medial wall of the frontal lobe that serves as the brain’s primary conflict-monitoring system. Its function is straightforward: when incoming information does not match existing predictions, the anterior cingulate cortex fires. It detects mismatch. It raises an alarm. And in people experiencing this pattern chronically, it is firing constantly.
The mismatch the anterior cingulate cortex registers is not between external reality and internal competence. The skill is often genuinely there. The mismatch is between the success signal coming in from the external environment (the promotion, the recognition, the degree, the title) and the self-model stored in memory, which does not include that level of achievement as a natural, expected outcome. The brain is not questioning your competence. It is questioning the accuracy of its own map.
This is a critical distinction. The brain has not detected an actual performance problem. It has detected a narrative discontinuity: a gap between who you have understood yourself to be and what reality is now presenting as evidence of who you are. The anterior cingulate cortex treats that gap as an error signal, and error signals in the brain are not neutral. They are motivating. They produce urgency, scanning behavior, and the compulsive need to resolve the mismatch before something goes wrong.
That urgency is what people experience as the anxiety underlying imposter syndrome. It is not anxiety about failure. It is the anxiety of an unsolved pattern-matching problem that the brain cannot let go of until it is resolved.
Why High-Achievers Are More Susceptible
There is something counterintuitive about this pattern being most prevalent among high-achievers, but the neuroscience makes it predictable. The same cognitive architecture that produces excellence also produces the conditions for it to take root.
High-achievers tend to hold internal standards that run significantly ahead of current performance. This is adaptive: it is the mechanism that drives continued improvement. But it also creates a permanent gap between self-evaluation and external validation. When external recognition arrives, the brain registers it as asynchronous with the internal standard. The achievement feels unreal because, by the internal measure that has always governed self-assessment, it arrived before the internal threshold was actually met.
The cognitive dissonance this produces is not trivial. The brain holds two simultaneous, contradictory representations: the external world’s assessment (which is positive) and the internal world’s assessment (which remains skeptical). Imposter syndrome is, in neurological terms, the experience of that dissonance before it has been resolved. High-achievers experience it more acutely because their internal standards are more demanding: the gap between where the internal bar sits and where external recognition is landing is simply wider.
There is also a second factor specific to high-performance environments: the density of competent peers. In a room where everyone is accomplished, the comparison set shifts. What felt like solid ground in a previous context becomes unremarkable in the new one. The brain’s threat-detection system interprets this recalibration as a warning, not that you don’t belong, but that the standards have changed and you may not have kept pace. In high-performance environments, this often manifests as the brain overcorrecting to a legitimate recalibration signal.
The Role of Attribution Style in Sustaining Imposter Feelings
The pattern persists, rather than resolving with accumulating evidence, because of a specific asymmetry in how the brain attributes outcomes. Successes are attributed externally: luck, timing, other people’s lowered expectations, being in the right place. Failures and near-misses are attributed internally: proof of the underlying inadequacy the person has always suspected. This attribution pattern is not random. It is a cognitively efficient way for the brain to maintain a stable self-model that has been organized around not-quite-enough.
The result is that evidence cannot accumulate in the way it theoretically should. Every piece of positive feedback is deflected before it can update the internal model. Every setback confirms what the model already predicted. This is not a problem of low self-esteem in the conventional sense. Many people experiencing these feelings function at a high level, present with appropriate confidence in professional contexts, and are well-regarded by their peers. The issue is narrower and more specific: an internally maintained self-model that was calibrated in a different context and has not been updated to reflect current reality.
The Neural Cost: Prefrontal Bandwidth and the Hidden Tax
The prefrontal cortex is the brain’s executive center: the region responsible for working memory, strategic planning, decision-making under uncertainty, and the flexible thinking that high-performance work demands. It is also, unfortunately, the same region that imposter syndrome colonizes.
The self-monitoring behavior it generates (the constant scanning for evidence that you are about to be found out, the rehearsal of explanations for why your success was unearned, the vigilant attention to how you are being perceived) all of this draws on prefrontal resources. The brain cannot fully allocate its executive capacity to the work at hand when a significant portion of that capacity is engaged in managing this narrative.
This is the mechanism behind the performance paradox that many people describe: working harder than anyone else, while simultaneously feeling less capable than everyone else, and producing work that is objectively good while experiencing it as perpetually insufficient. The effort is real. The output is real. But the neural overhead is also real, and it is coming at a cost that, over time, accumulates into something closer to genuine cognitive depletion than ordinary professional stress.
Prefrontal capacity consumed by self-monitoring is prefrontal capacity that is not available for creative synthesis, for the kind of integrative thinking that produces genuine insight, or for the confident forward-movement that high-stakes decisions require. This does not just feel exhausting: it is neurologically expensive. The experience of being drained, of working twice as hard for the same output, is not a perception distortion. It reflects a genuine division of cognitive resources.
The Physiological Amplifier
When imposter syndrome triggers the anterior cingulate cortex’s error-detection system, the body’s stress response follows. Cortisol rises. The amygdala, the brain’s alarm center, becomes more reactive. The threshold for perceiving threat drops. What this means in practice is that a casual question from a senior colleague, a moment of hesitation in a presentation, a critical email, stimuli that a brain in a baseline state would process and move on from, are now processed as potential exposures, potential confirmations of the feared inadequacy.
The heightened amygdala reactivity that accompanies this pattern creates a feedback loop: the stress response narrows perception, which increases the frequency of threat-detection events, which sustains the stress response. This is the same emotional resilience and regulation architecture that governs how the brain processes sustained threat under pressure. People in this loop often report that the experience is worst precisely when the stakes are highest, in the rooms and situations where their full cognitive capacity is most needed.
Imposter Feelings Versus Genuine Skill Gaps: The Accuracy Problem
One of the more practically important distinctions in understanding imposter syndrome is separating the experience of perceived inadequacy from the reality of actual skill gaps. These are not the same thing, and treating them as equivalent leads to responses that are mismatched to the actual problem.
Genuine skill gaps produce specific, locatable deficits. There is a task, a knowledge domain, or a capability that is genuinely underdeveloped, and the person can usually identify it with some precision when pressed. The response to a genuine skill gap is skill acquisition, and when skill acquisition happens, the feeling of inadequacy in that domain reduces proportionally. The system is functioning correctly.
This pattern does not work that way. The feeling of inadequacy does not track actual skill level. People with extensive, demonstrably sufficient competence experience it. They experience it after acquiring new skills. They experience it after receiving strong positive feedback. The inadequacy signal does not diminish when competence increases, because it was never accurately tracking competence in the first place. It was tracking the gap between the external signal and the internal self-model, and that gap persists until the self-model is updated, regardless of what happens to actual skill level.
This distinction matters enormously in practice. The person who responds to these feelings by acquiring more credentials, more knowledge, more proof, is solving the wrong problem. More evidence does not update a self-model that has been organized to deflect evidence. The issue is not with the evidence. It is with the cognitive architecture that is processing it.
Self-Assessment Accuracy and the Dunning-Kruger Inversion
Research on self-assessment accuracy consistently shows that the most skilled people in a domain tend to underestimate their relative performance, while the least skilled tend to overestimate it. This is not accidental. Expertise creates the capacity to perceive complexity: to see what you do not yet know, what could be done better, where the current work falls short of the ideal. The more deeply someone understands a field, the more clearly they can see the distance between where they are and where the frontier of that field actually sits.
The imposter narrative often rides this dynamic. The person experiencing it is, in many cases, genuinely perceptive about the gap between their current performance and the best possible performance. What the narrative distorts is the inference drawn from that accurate perception. The accurate reading, “I can see that this work could be better”, becomes the distorted conclusion: “I am not qualified to be doing this work.” The perception is real. The conclusion is a cognitive error generated by a self-model that has not been updated to include the person’s current level of development.
Dr. Ceruto’s Real-Time Intervention Approach
Dr. Sydney Ceruto’s work with imposter syndrome operates at the level of the neural architecture that generates it, not the surface-level content of the narrative, but the underlying pattern that keeps producing it. Her approach is built on a foundational principle: the brain is not a fixed system. Neural pathways that have been organized around a particular self-model can be reorganized. The self-model can be updated. And when it is updated at the level of the neural circuitry that maintains it, the change is not an intellectual reframing: it is a structural shift in how the brain processes identity-relevant information.
The real-time component of her approach is specifically designed to address the moment when this pattern is most active: during high-stakes performance, in the rooms and situations where the neural cost is being paid most acutely. Rather than working in the abstract, between episodes, her methodology engages the pattern at the moment it fires, using the brain’s own plasticity mechanisms to interrupt the anterior cingulate’s error signal before it cascades into the full response.
The goal is not to silence self-monitoring: self-monitoring is useful and adaptive in its appropriate register. The goal is to recalibrate what the self-monitoring system is tracking. When the internal self-model is updated to accurately reflect current competence and context, the anterior cingulate cortex’s error-detection function stops generating false alarms. The vigilance dissolves, not because it has been suppressed, but because the mismatch it was responding to no longer exists.
What this looks like in practice is a systematic process of identity-level updating: not affirmations layered over an unchanged self-model, but genuine revision of the neurological architecture that holds the self-model in place. The work addresses the attribution asymmetry that prevents positive evidence from accumulating, the comparison frameworks that sustain the sense of inadequacy in high-performance environments, and the stress-response amplification that makes the experience most disabling precisely when full cognitive capacity is most needed. At its core, imposter syndrome is a disruption of identity and neural flexibility: the brain’s self-model has calcified around outdated information.
For people who have been living with imposter syndrome for years (who have accumulated degrees, promotions, and recognition while the internal narrative has remained unchanged) this approach offers something different from the conventional responses. It works at the level where the problem actually lives. If you are ready to address this at that level, the next step is to schedule a strategy call with Dr. Ceruto directly.
The Forward Question
Imposter syndrome is a coherent, neurologically explicable response to a specific set of conditions. Understanding those conditions (the anterior cingulate’s error-detection function, the self-model’s resistance to updating, the prefrontal cost of sustained self-monitoring) does not make imposter syndrome less real. But it does make the path through it significantly clearer.
The question this pattern raises is not whether you are actually capable. The evidence on that question has typically been accumulating for years. The real question is whether your neural architecture is organized to receive that evidence: to let it update the self-model that was built in an earlier context and has been generating false alarms ever since.
When the self-model is updated, the pattern does not gradually fade. It resolves. The vigilance that was consuming prefrontal bandwidth is freed for actual work. The attribution asymmetry that was deflecting positive evidence corrects. The stress-response amplification that was narrowing perception at the worst possible moments quiets. What remains is a brain that is no longer working against itself: one that can bring its full capacity to bear on the work that has been waiting for it all along.