Your nervous system is not reacting to your life. It is running a program that was written long before you had any say in the matter, and that program is determining which version of you shows up in every conversation, every decision, every moment of pressure. The autonomic nervous system operates beneath conscious awareness, governing heart rate, respiratory rhythm, digestive function, and the speed at which your prefrontal cortex can access its own resources. When this system is well-calibrated, you experience flexible autonomic regulation: the capacity to escalate arousal when a situation demands it and return to baseline when the demand passes. When it is not, you live in a body that is perpetually braced for something that may or may not arrive.
In my practice, the individuals who come to me with nervous system dysregulation rarely describe it in neurological terms. They describe a sense that they cannot fully relax, that their sleep is unrepairing, that their emotional reactions are disproportionate to their triggers, that they are simultaneously exhausted and wired. These are not psychological complaints. They are the behavioral signatures of an autonomic system that has lost its capacity to shift states accurately. This page brings together 12 articles from the MindLAB library exploring the architecture of nervous system regulation and the methodology I use to restore autonomic precision.
The Autonomic Nervous System Is an Architecture, Not a Switch
The most common misunderstanding about the autonomic nervous system is that it operates as a binary: sympathetic activation on one side, parasympathetic recovery on the other, and health is a matter of tipping the balance toward calm. This model is intuitive and incomplete. The autonomic nervous system is not a seesaw. It is a multi-layered regulatory architecture in which both branches operate simultaneously, in varying ratios, across every organ system in your body.
Sympathetic activation does not mean panic. It means mobilization: the allocation of metabolic resources toward action. Parasympathetic activation does not mean relaxation. It means restoration: the direction of resources toward digestion, tissue repair, immune surveillance, and memory consolidation. A well-regulated nervous system transitions fluidly between them, matching physiological state to environmental demand with precision.
What I consistently observe in high-performing individuals is not an absence of sympathetic capacity: they have enormous reserves for mobilization. The breakdown is in the transition. They can escalate. They cannot de-escalate on cue. The autonomic flexibility that would allow them to shift from a high-stakes meeting to a quiet dinner with their family in 20 minutes has been eroded by months or years of sustained activation. The nervous system has learned that the safest default is readiness, and it no longer trusts the signal that says the demand has passed.
Polyvagal Theory: Three States, Not Two
Stephen Porges’s polyvagal theory reframed the neuroscience of autonomic regulation by identifying not two but three hierarchically organized states within the autonomic nervous system. This framework has become foundational in my practice because it explains patterns of behavior that the traditional sympathetic-parasympathetic binary cannot account for.
The three states, organized from most recently evolved to most primitive:
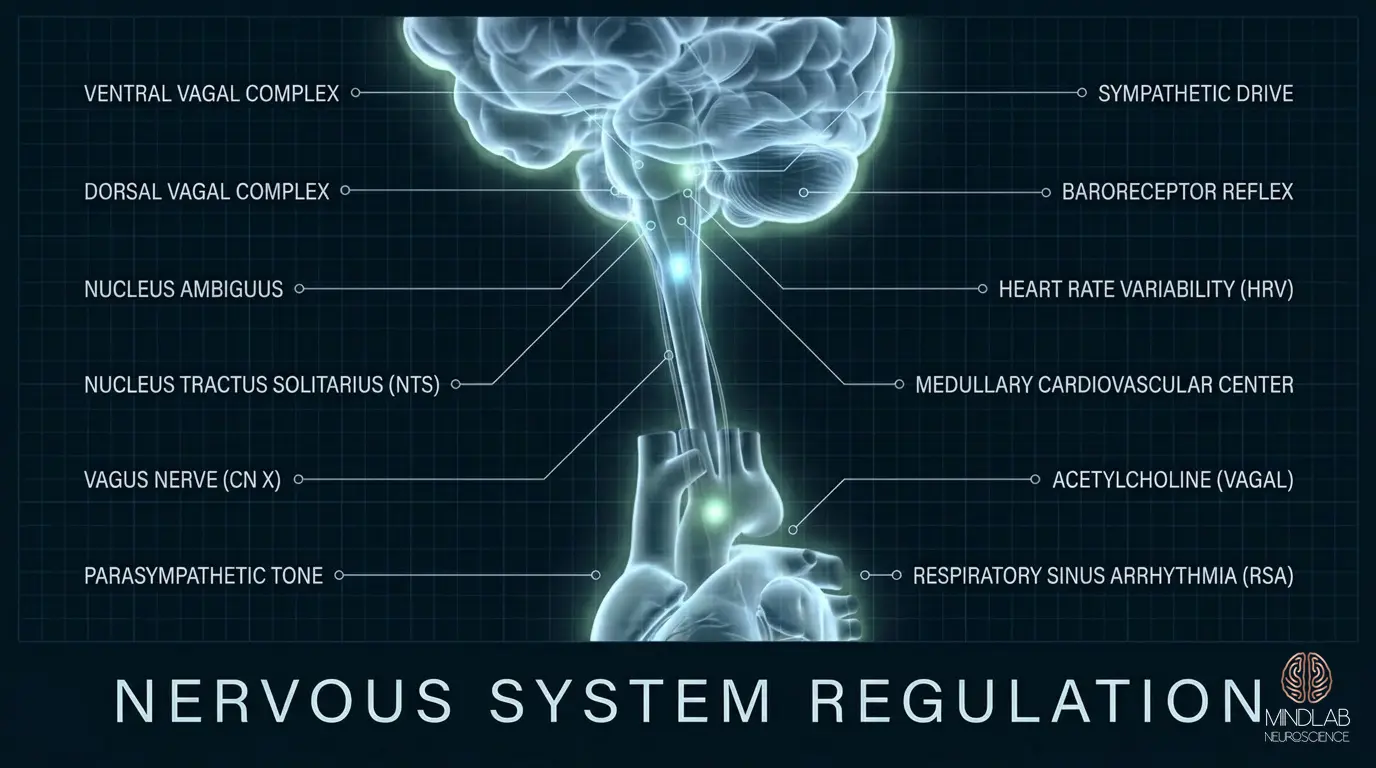
Ventral vagal activation: the social engagement system. Governed by myelinated vagal fibers originating in the nucleus ambiguus, this state supports connection, communication, prosodic voice modulation, and the capacity to remain present during complex interpersonal exchanges. This is not a state of calm. It is a state of flexible, socially engaged readiness.
Sympathetic mobilization: the fight-or-flight architecture. When the nervous system detects a threat that ventral vagal resources cannot manage, it shifts to sympathetic dominance: elevated heart rate, cortisol and adrenaline release, blood flow redirection to skeletal muscles. Designed to be temporary: a high-energy response that resolves when the threat passes.
Dorsal vagal shutdown: the freeze and collapse response. Governed by unmyelinated vagal fibers originating in the dorsal motor nucleus, this is the nervous system’s oldest defensive state. When neither engagement nor mobilization resolves the threat, it defaults to immobilization: reduced heart rate, metabolic conservation, emotional flatness, dissociative features. In modern terms, it is the numbness and cognitive shutdown that individuals describe as “checking out.”
The critical insight from polyvagal theory is that these states are not choices. They are neuroceptive responses: automatic evaluations of safety and threat conducted by neural circuits below conscious awareness. A person cannot will themselves from dorsal vagal collapse into ventral vagal engagement. The intervention must occur at the level of the neural circuitry that governs state transitions, not at the level of conscious intention.
Heart Rate Variability: The Biomarker Your Nervous System Is Broadcasting
Heart rate variability (HRV) is the measurable variation in time intervals between consecutive heartbeats, and it is the single most informative biomarker of autonomic regulatory capacity available outside a laboratory. A heart that beats at a perfectly metronomic 70 beats per minute is not a healthy heart: it is a heart whose autonomic input has lost its variability. Higher HRV reflects robust vagal tone and a nervous system capable of rapid, flexible adjustments to changing demands.
The physiology is precise. On each inhalation, sympathetic influence slightly accelerates heart rate. On each exhalation, parasympathetic input via the vagus nerve decelerates it. This beat-to-beat fluctuation, respiratory sinus arrhythmia, is a direct readout of vagal brake function. Research published in Biological Psychology has repeatedly demonstrated that low resting HRV is associated with reduced emotional regulation capacity, impaired cognitive flexibility, and increased vulnerability to stress-related conditions.
In my practice, I use HRV data not as a wellness metric but as a neural diagnostic signal. An individual’s HRV pattern over days and weeks reveals the autonomic story that self-report cannot capture. I have worked with clients who report feeling “fine” while their HRV data shows sustained sympathetic dominance with virtually no parasympathetic recovery signature: a nervous system running at mobilization intensity around the clock without registering the cost consciously.
The Autonomic Ladder and the Window of Tolerance
Dan Siegel’s concept of the window of tolerance describes the zone of arousal within which an individual can experience emotional activation (stress, frustration, excitement, grief) without losing access to prefrontal executive function. Inside the window, you can feel intensely and still think clearly. Outside it, one of two things happens: hyperarousal (sympathetic flooding) or hypoarousal (dorsal vagal collapse).
What determines the width of your window is not your psychological resilience. It is the calibration precision of your autonomic nervous system. An individual with robust vagal tone has a wide window: they can tolerate significant activation without losing executive function. An individual whose nervous system has been shaped by sustained stress or chronic threat signaling has a narrow window: they shift into hyperarousal or hypoarousal at relatively low thresholds.
The autonomic ladder maps these transitions. At the top: ventral vagal engagement, full cognitive and emotional resources. One rung down: sympathetic activation, mobilization without collapse. At the bottom: dorsal vagal shutdown. In my practice, I observe that most clients oscillate, cycling between sympathetic hyperactivation and dorsal vagal flatness, rarely spending sustained time in the ventral vagal state where their highest-order functioning lives. The nervous system is trapped in a loop between two defensive states, bypassing the state that would actually serve them.
This oscillation is a failure of neuroceptive threshold calibration: the thresholds were set by experience, often early experience, and they operate automatically. Changing them requires intervention at the level of the vagal circuitry itself.
Why Breathing Exercises Alone Do Not Restructure the System
Controlled breathing is the most commonly prescribed intervention for nervous system regulation, and it is not wrong: it is insufficient. Slow, extended-exhalation breathing does activate the vagal brake, shifting autonomic balance toward parasympathetic influence in the moment. Cardiac coherence research confirms acute, measurable effects on HRV during deliberate respiratory protocols.
The limitation is structural. A breathing exercise produces a temporary parasympathetic shift. It does not alter the baseline autonomic set point that the nervous system returns to when the exercise ends. For an individual whose autonomic system has been calibrated to chronic sympathetic dominance over months or years, breathing exercises are analogous to manually overriding a thermostat for 10 minutes: the temperature shifts briefly, and the system reverts to its programmed setting.
In my practice, I have worked with hundreds of individuals who have diligently practiced breathwork, yoga, and vagal nerve stimulation techniques, and who remain chronically dysregulated. They are not doing the exercises wrong. The exercises are producing temporary state shifts. What they are not doing is rewiring the default mode of the autonomic nervous system: the baseline setting to which the system returns between interventions. That rewiring requires targeting the neural patterns driving the dysregulation, not the physiological symptoms downstream of it.
Chronic Dysregulation in High-Performers: The Hidden Cost
The individuals I work with are not fragile. They are among the highest-functioning people in their fields: executives, founders, surgeons, trial attorneys, professional athletes. And yet, when I assess their autonomic profiles, a consistent pattern emerges: chronic sympathetic dominance masked by extraordinary compensatory capacity. They have been running their nervous systems at mobilization intensity for so long that they have mistaken the activation for their natural operating state.
The compensation is real and measurable. High performers develop what I call cortical override patterns: the prefrontal cortex learns to suppress the behavioral signals of autonomic distress, maintaining outward composure, decision quality, and social engagement even while the underlying nervous system is in sustained fight-or-flight. This is not the same as regulation. It is suppression. And suppression has a metabolic cost that compounds over time.
The cost manifests along predictable pathways. Sleep architecture degrades first: the nervous system cannot enter deep restorative stages because sympathetic tone remains elevated during the night, disrupting the slow-wave and REM cycles that govern neural repair and memory consolidation. Immune function shifts next: chronic sympathetic activation suppresses natural killer cell activity and shifts cytokine profiles toward pro-inflammatory patterns, as documented in Segerstrom and Miller’s meta-analysis in Psychological Bulletin. Cognitive precision erodes third: prefrontal-amygdala connectivity weakens under sustained stress, an effect driven mainly by excessive catecholamine signaling and amplified by cortisol, reducing the executive function that these individuals depend on for their professional identity.
What makes this pattern particularly insidious is that high performers typically do not seek help until the compensatory system itself begins to fail. The first sign is often not anxiety or emotional distress: it is a cognitive symptom: word-finding difficulty, slower processing speed, impaired working memory under pressure. They describe it as “losing their edge.” What they are actually experiencing is the prefrontal cortex losing its capacity to override an autonomic system that has been in sustained distress for years. The override was never a solution. It was a loan against future neural resources, and the debt is now coming due.
Dr. Ceruto’s Approach to Autonomic Recalibration
My approach to nervous system regulation begins with a premise that separates it from every breathing app, yoga protocol, and somatic experiencing framework available: the autonomic nervous system’s baseline calibration is a product of neural patterning, and neural patterns can be structurally rewired. Not managed. Not coped with. Rewired.
The first phase of autonomic recalibration in my practice is precision mapping. I identify the specific neuroceptive triggers: the environmental, relational, and internal cues that the nervous system has learned to interpret as threat signals. These triggers are highly individual. For one client, it is the sound pattern of a particular vocal tone that activates sympathetic mobilization. For another, it is the proprioceptive sensation of being in an enclosed space with multiple people. For a third, it is the cognitive detection of ambiguity in a professional communication: the nervous system has learned to treat uncertainty as danger. Each trigger maps to a specific neural circuit, and each circuit has a specific intervention architecture.
The second phase targets vagal tone restoration at the level of the dorsal motor nucleus and nucleus ambiguus: the brainstem structures that govern the vagus nerve’s regulatory output. This is not achieved through conscious breathing alone. It requires sustained engagement with the neural safety signals that activate the ventral vagal system: co-regulation with a trusted nervous system (which is one reason the relationship between practitioner and client is not incidental to this work: it is neurologically essential), progressive exposure to emotional resilience and autonomic flexibility demands within a regulated relational context, and real-time interruption of the sympathetic escalation patterns at the moment they activate.
Real-Time Neuroplasticity™ is particularly effective for autonomic work because the nervous system’s patterns fire fastest and most automatically under actual conditions of activation, not during calm reflection about activation. A pattern that is interrupted and replaced while the nervous system is actively firing produces structural change at the synaptic level. A pattern that is discussed retrospectively produces insight. Insight is valuable. It is not rewiring.
The third phase addresses what I call autonomic identity reconstruction: the process by which the nervous system learns to recognize a new baseline as safe. This is the phase most approaches skip entirely. Even when acute dysregulation is reduced, the nervous system’s default calibration may still be set to a state of low-grade mobilization. The individual feels “better” but never fully at ease. Their HRV improves but plateaus below optimal. Their window of tolerance widens but remains narrower than their cognitive capacity would predict. Full recalibration requires the nervous system to update its definition of baseline safety, and that update only occurs through sustained, repeated experience of regulated activation within the stress and nervous system regulation architecture that governs state transitions.
The Nervous System Does Not Forget, But It Can Be Retrained
One of the most important concepts I communicate to every individual I work with on autonomic regulation is this: the nervous system’s current calibration is not a malfunction. It is an adaptation. A system that defaulted to sympathetic dominance did so because, at some point in the individual’s history, sustained vigilance was the most adaptive response available. The dorsal vagal shutdown that produces numbness and disconnection was, in its original context, a survival mechanism. The narrow window of tolerance was protective before it became restrictive.
Understanding this changes the entire orientation of the work. We are not fighting the nervous system. We are updating it, providing it with new data about the current environment that contradicts the threat model it has been operating from. This is neuroplasticity applied to autonomic architecture: the same capacity for experience-dependent synaptic modification that allows the cortex to learn a new language or acquire a new skill also allows the brainstem and vagal circuits to recalibrate their threat-response thresholds.
Research from Porges and Dana, published in Frontiers in Integrative Neuroscience, has demonstrated that sustained co-regulatory experience (repeated, reliable engagement with a nervous system that signals safety) can shift neuroceptive thresholds over time, effectively expanding the window of tolerance by resetting the autonomic ladder’s trigger points. This is the neural mechanism underlying what my clients experience as a fundamental shift in how they move through their lives: not the absence of stress, but the return of the capacity to meet stress without losing access to their own cognitive and emotional resources.
The articles on this page explore every dimension of this architecture: the vagus nerve and polyvagal dynamics that govern autonomic state transitions, the relationship between HRV and regulatory capacity, the neuroscience of why high performers are particularly vulnerable to masked dysregulation, and the specific methodology I use to produce durable autonomic change. If what you have read here maps onto your own experience (if you recognize the pattern of sustained activation, compensatory override, and a nervous system that never fully settles) I invite you to schedule a strategy call with Dr. Ceruto. That conversation is the beginning of identifying exactly where in your autonomic architecture the recalibration needs to occur, and what the pathway to restored regulation looks like for your specific neural profile.