When you start managing your parent’s medications, finances, and safety, your brain is not simply taking on tasks. It is running a template in reverse. The attachment circuitry built in childhood to receive care now has to deliver it, and that inversion, sustained under chronic stress, is what reshapes the caregiver brain.

Key Takeaways
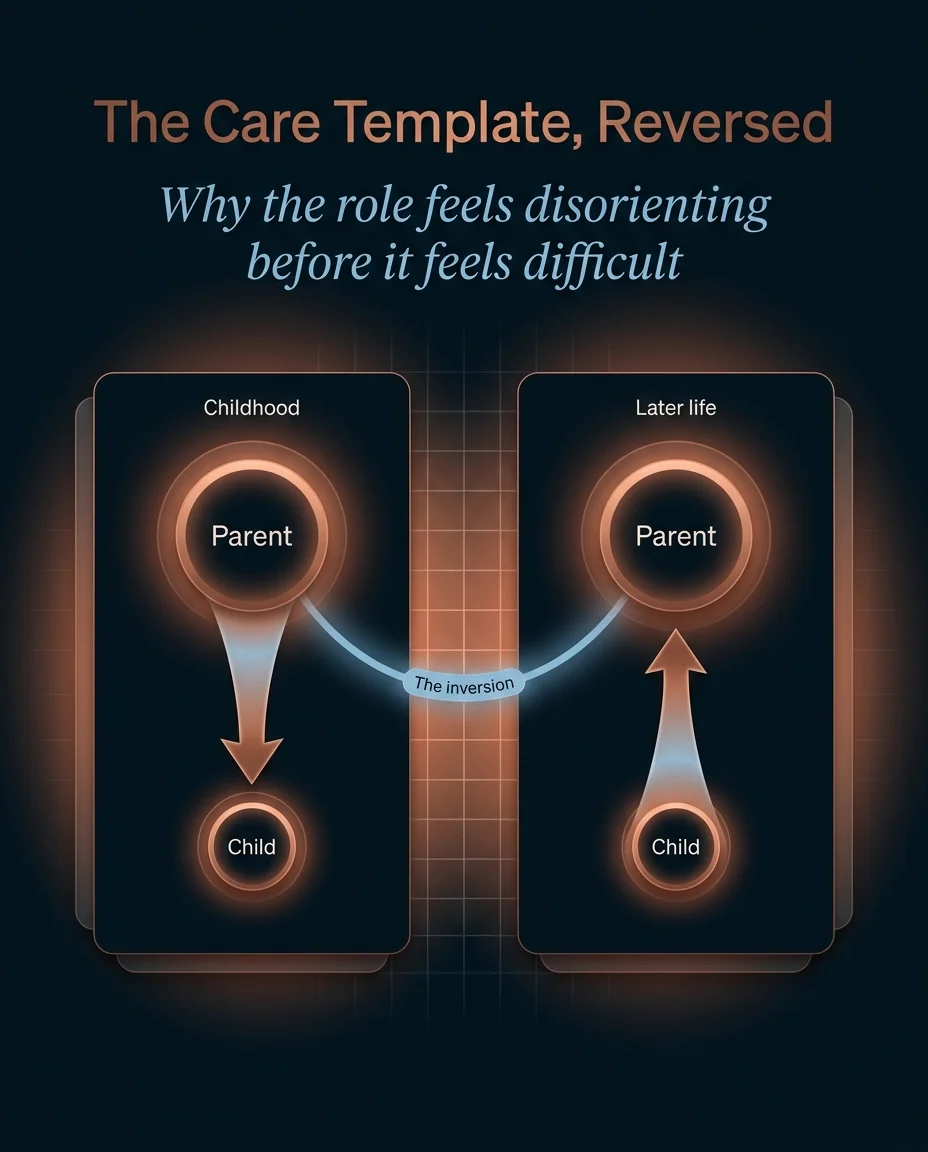
- Becoming your parent’s caregiver inverts the attachment template the brain encoded in childhood, which is why the role can feel disorienting long before it feels difficult.
- Caregiver burnout is a chronic-stress-circuit pattern, not a willpower failure: sustained cortisol load measurably wears on the prefrontal cortex and hippocampus while the threat-sensitive amygdala grows.
- Grief frequently arrives before the loss does, because the brain registers the gap between the parent you have now and the parent encoded in memory.
- Across a UK population study of more than 2,600 adults, caregivers carried significantly higher allostatic load, a cumulative physiological stress measure that predicts later illness and disability.
- Protecting your own nervous system is not optional self-care layered on top of the role. It is the mechanism that keeps the role survivable.
What happens in the brain when you start parenting your own parent?
The disorientation that adult children describe when a parent begins to decline is not vague emotion. It is the felt sense of a neural template inverting. From infancy, the attachment system wires a specific direction of care: the parent is the secure base, the source of regulation and safety, and the child’s nervous system learns to turn toward that figure under threat. The strength of that early bond, shaped in relationships like the neuroscience of the mother-daughter relationship, is part of what makes its later inversion so disorienting. Decades later, that wiring does not simply switch off because circumstances change.
Developmental researchers describe the transition into the caregiving role as filial maturity, a stage in which the adult child accepts that the parent now needs support and begins to relate to them beyond the strictly parental frame. In one study of 304 adult children caring for parents aged sixty-five and over, attachment style and a person’s internal model of caregiving together explained roughly a quarter of the variation in how fully they comprehended the new role, which signals just how much of this transition runs on attachment circuitry rather than logistics alone (Morais et al., 2024). In my practice, the clients who struggle most with this shift are rarely the ones with the heaviest practical load. They are the ones whose self-concept is most tightly bound to the parent who is now changing.
This is the same template-encoding mechanism that runs throughout the neuroscience of family systems, where close relatives become wired into how we see ourselves. In its most fused form the bond can blur where one person ends and another begins, a pattern explored in the neuroscience of enmeshment in families. The caregiving inversion does not erase that wiring. It demands that the wiring run backward, and the brain treats that reversal as significant.
What looks like a character failure is the predictable signature of a brain under sustained allostatic load.
– Dr. Sydney Ceruto
Why does caregiver burnout look like a stress-circuit problem, not a willpower problem?
Caregiver burnout is one of the most misread patterns in family life. The exhaustion, the shortened fuse, the difficulty concentrating, the sense of running on empty: these read culturally as personal weakness, as if a more disciplined person would simply cope. The neuroscience says otherwise. What looks like a character failure is the predictable signature of a brain under sustained allostatic load.
Allostatic load is the cumulative wear that accrues when the body’s stress-response systems stay switched on too long. Chronic activation keeps cortisol and related mediators elevated, and the brain pays a structural price. Repeated stress drives atrophy of neurons in the prefrontal cortex and hippocampus, the regions responsible for executive function, working memory, and selective attention, while the amygdala, the brain’s threat-and-vigilance center, grows more reactive (McEwen, 2017). That is a precise map of the caregiver’s experience: harder to plan, harder to hold details, harder to stay calm, easier to feel under threat.
This is not a fringe finding. In a population-based study comparing 471 caregivers with more than 2,100 non-caregivers, caregivers showed significantly higher allostatic load, and that elevated load predicted future illness and disability (Gallagher et al., 2021). The physiological cost compounds over time. The classic work on caregiving and cellular aging found that women under the highest chronic stress had telomeres shorter by the equivalent of at least a decade of additional aging compared with low-stress peers (Epel et al., 2004). When a caregiver tells me they feel like they have aged years in months, they are often describing something biologically real.
Reframing burnout as a circuit-level pattern rather than a personal deficit changes what to do about it. You cannot discipline a depleted prefrontal cortex into working harder. You can, however, change the inputs that are loading the circuit, which is the same logic that governs how cortisol moves between family members and what it takes to interrupt the load. It is one expression of the broader architecture of how relationship patterns are wired into the brain.
Why does grief arrive before the loss does?
One of the most isolating parts of this role is grieving someone who is still alive. Adult children often feel they have no right to mourn a parent who is sitting across the table, and yet the sadness is real and recurring. This is anticipatory grief, and it is not a sign of giving up early. It is an active psychological process the brain runs in response to a widening gap between the parent encoded in long-term memory and the parent in front of you.
Research on family caregivers of relatives with progressive cognitive decline finds that anticipatory grief is common, intensifies as the condition advances, and is closely tied to caregiver burden (Pérez-González et al., 2023). Crucially, it is distinct from simply anticipating a death. The brain is mourning the loss of a relationship in its prior form, a loss that is happening continuously rather than at a single moment. Neuroimaging work on dementia caregivers has begun to identify the neural signatures associated with how grief resolves over time, underscoring that this is a brain process with measurable correlates, not merely a mood (Jain et al., 2019). One additional study examining caregivers across the course of the condition reported that anticipatory grief was widespread in the sample and rose alongside the severity of the parent’s decline (Pérez-González et al., 2021).
Naming this pattern matters because unrecognized grief does not disappear. It leaks into irritability, guilt, and a sense that something is wrong with you for feeling it. There is nothing wrong with you. Your brain is doing exactly what an attachment system does when the figure it is bonded to is changing in front of it.

You cannot discipline a depleted prefrontal cortex into working harder.
– Dr. Sydney Ceruto
How do you protect your own nervous system while carrying the role?
If burnout is a loading problem, then the intervention is not to summon more willpower but to change how the circuit is being loaded and to build in genuine recovery. This is where I work with caregiving clients directly, because the generic advice to practice self-care almost always fails: it treats recovery as a luxury to fit in after everything else, which is exactly backward.
The first principle is to treat nervous-system recovery as load-bearing infrastructure, not a reward. Brief, reliable periods in which the stress response is allowed to switch off do more for prefrontal function than occasional large breaks that never arrive. The second principle is to make the attachment inversion explicit rather than letting it run as a silent expectation. When an adult child can name that they are running a reversed care template, the guilt that drives over-functioning loosens, because the standard they are failing to meet was never realistic to begin with. The third principle is to distribute load deliberately, including across siblings, before the system reaches overload rather than after, since the structural arrangement of who carries what is one of the few inputs a caregiver can actually change.
None of this removes the difficulty of the role. What it does is keep the difficulty from compounding into the structural brain changes that chronic, unrelieved stress produces. The goal is not to feel nothing. The goal is to keep the caregiver’s own neural architecture intact while they carry something genuinely hard.
Understanding the mechanism is the first move. Translating it into a plan that fits your specific family system is the next one, and it is the work itself rather than information that protects the caregiver’s nervous system.
There is nothing wrong with you. Your brain is doing exactly what an attachment system does when the figure it is bonded to is changing in front of it.
– Dr. Sydney Ceruto
- Morais, D., Faria, C., & Fernandes, L. (2024). Filial Maturity and Caregiving to Aging Parents. Geriatrics, 9(1), 17. https://doi.org/10.3390/geriatrics9010017
- McEwen, B. S. (2017). Neurobiological and Systemic Effects of Chronic Stress. Chronic Stress, 1. https://doi.org/10.1177/2470547017692328
- Gallagher, S., et al. (2021). Caregiving and allostatic load predict future illness and disability: A population-based study. Brain, Behavior, & Immunity – Health, 16, 100295. https://doi.org/10.1016/j.bbih.2021.100295
- Epel, E. S., et al. (2004). Accelerated telomere shortening in response to life stress. Proceedings of the National Academy of Sciences, 101(49), 17312–17315. https://doi.org/10.1073/pnas.0407162101
- Pérez-González, A., Vilajoana-Celaya, J., & Guàrdia-Olmos, J. (2023). Burden and anticipatory grief in caregivers of family members with Alzheimer’s disease and other dementias. Palliative & Supportive Care, 22(5). https://doi.org/10.1017/S1478951523001360
- Jain, F. A., et al. (2019). Grief, Mindfulness and Neural Predictors of Improvement in Family Dementia Caregivers. Frontiers in Human Neuroscience, 13, 155. https://doi.org/10.3389/fnhum.2019.00155
- Pérez-González, A., Vilajoana-Celaya, J., & Guàrdia-Olmos, J. (2021). Alzheimer’s Disease Caregiver Characteristics and Their Relationship with Anticipatory Grief. International Journal of Environmental Research and Public Health, 18(16), 8838. https://doi.org/10.3390/ijerph18168838
The role reversal with an aging parent is one of the most demanding transitions a family system goes through, and it rewires the people inside it. Working with the neuroscience, rather than against it, is what makes the role sustainable.
Frequently Asked Questions
Is it normal to feel resentment toward a parent I am caring for?
Yes, and it does not mean you love them less. Resentment under caregiving is a predictable output of a stress-loaded nervous system combined with an attachment template that is running in reverse. The brain that is depleted and vigilant produces irritability and resentment as symptoms of load, not as evidence of a flaw in your character.
Why do I grieve my parent when they are still alive?
This is anticipatory grief, an active process the brain runs when the parent in front of you no longer matches the parent stored in your memory. Research on family caregivers shows it is common and tends to deepen as a parent’s decline progresses. It is mourning a relationship that is changing in real time, which is a real loss even though no death has occurred.
Why does caregiving split siblings apart?
Because the load is rarely shared evenly, and because each sibling enters the role carrying a different childhood template of the same parent. When one sibling absorbs most of the practical and emotional weight, the resulting strain interacts with old family roles and can reactivate patterns set decades earlier. Distributing load deliberately and early is one of the few structural inputs that reliably reduces the conflict.
How do I protect my own health while caring for my parent?
Treat nervous-system recovery as essential infrastructure rather than an optional reward. Brief, reliable periods where the stress response can switch off protect prefrontal function more than rare large breaks. Because chronic caregiving stress carries measurable physiological cost, including elevated allostatic load, protecting recovery is a health intervention, not an indulgence.
When should I seek outside support for the caregiving role?
When the load has started to change how your brain functions day to day, persistent difficulty concentrating, a constantly short fuse, sleep that no longer restores you, these are signals that the stress circuit is overloaded rather than that you are failing. That is the point to bring in structured support, which can include mapping your own nervous-system response so the role becomes survivable.