Why Emotional Resilience Is a Neural Architecture Problem
Emotional resilience is not what most people think it is. It is not a personality trait. It is not the capacity to endure suffering without complaint, and it is absolutely not the product of willpower or positive thinking. In 26 years of working with individuals who operate under extraordinary pressure (executives navigating organizational crises, founders absorbing the psychological weight of companies that depend on their decisions, partners trying to rebuild trust after relational rupture) what I consistently observe is that the people who recover from adversity and the people who don’t are not separated by character. They are separated by neural architecture.
The neuroscience of emotional resilience has fundamentally rewritten our understanding of what it means to withstand difficulty and re-engage with life after disruption. Resilience is not bouncing back. It is the brain’s capacity to maintain functional connectivity between the structures that register threat and the structures that regulate the response, and that connectivity is measurable, modifiable, and, critically, trainable.
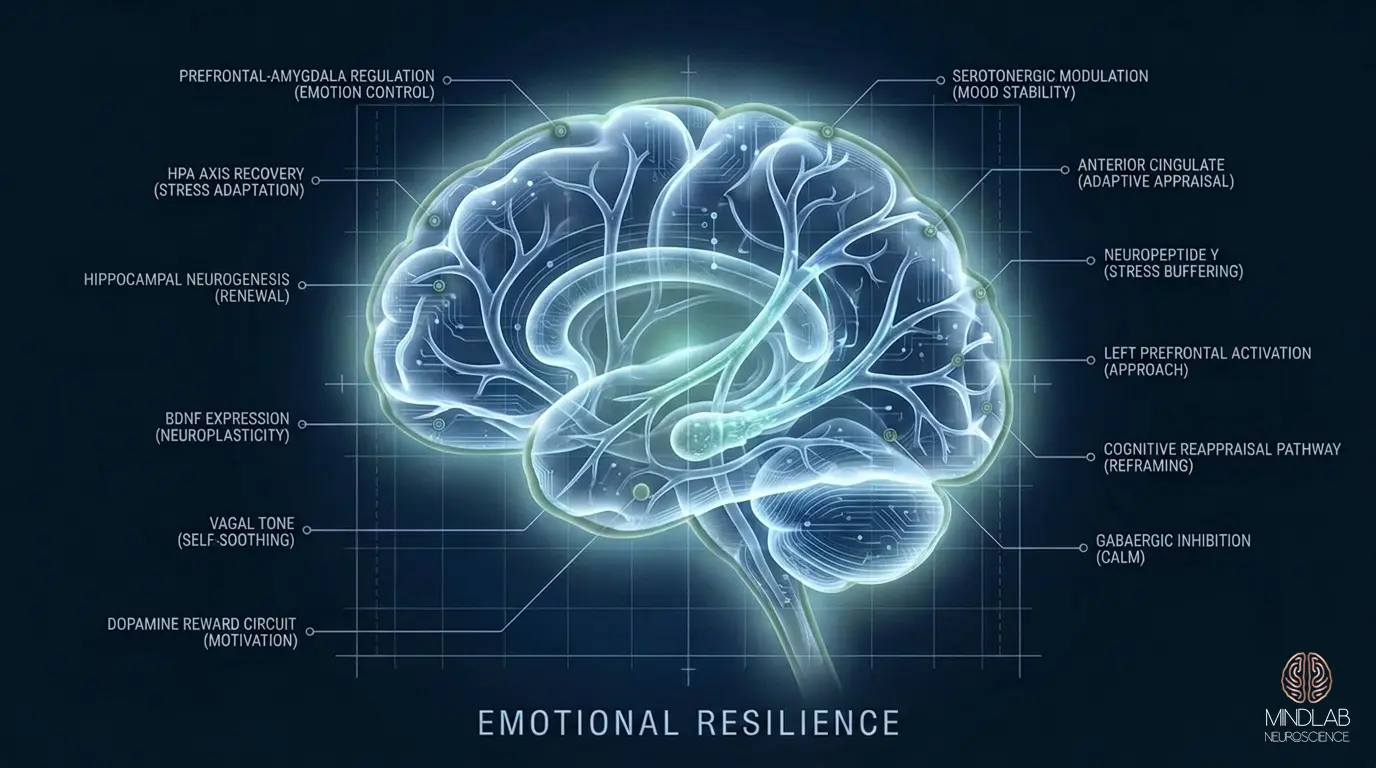
The central circuit is the prefrontal-amygdala pathway. When this pathway is robust, the prefrontal cortex can modulate the amygdala’s threat signal in real time, not eliminating the response, but calibrating its intensity and duration to match the actual demands of the situation. When this pathway is degraded (through chronic stress, traumatic encoding, or insufficient recovery) the amygdala fires without adequate prefrontal regulation, and the individual experiences what feels like emotional collapse but is actually a connectivity problem at the circuit level.
The Prefrontal-Amygdala Circuit: Where Resilience Lives
If you wanted to locate resilience in the brain, you would not find it in a single structure. You would find it in the quality of communication between structures: specifically in the bidirectional signaling between the medial prefrontal cortex and the amygdala.
The medial prefrontal cortex, particularly the ventromedial prefrontal cortex and the prelimbic region, serves as the brain’s executive regulator of emotional responses. It receives information from the amygdala about threat detection and sends inhibitory signals back, effectively telling the amygdala whether the detected threat warrants a full activation cascade or whether the situation can be managed without mobilizing the entire stress response system. Research by neuroscientist Gregory Quirk and others has demonstrated that the strength of this top-down inhibitory projection is one of the most reliable neurobiological predictors of how an individual will respond to adversity.
In individuals with high resilience, this pathway is characterized by dense connectivity, rapid signaling, and efficient inhibitory regulation. The amygdala still detects the threat: resilience does not mean the brain ignores danger, but the prefrontal cortex responds with precision rather than delay. The threat is registered, evaluated, and contextualized before the full physiological cascade deploys.
In individuals with low resilience, the pathway shows reduced connectivity. The prefrontal signal arrives late, arrives weakly, or fails to override the amygdala’s initial activation. The result is a disproportionate stress response, an intensity and duration that exceeds what the situation demands, and a recovery period that extends far longer than it should. This is not a failure of character. It is a circuit-level deficit that has identifiable neuroanatomical correlates and, because of neuroplasticity, identifiable solutions.
Allostatic Load: The Neuroscience of the Breaking Point
Every brain has a threshold beyond which its regulatory systems begin to degrade under sustained demand. The neuroscientist Bruce McEwen termed this accumulation of physiological wear allostatic load: the total cost of maintaining stability in the face of repeated or chronic stress. Understanding allostatic load is essential for understanding resilience, because resilience failure is not usually the product of a single catastrophic event. It is the product of accumulated load exceeding the system’s capacity to recover between demands.
The HPA axis, the hypothalamic-pituitary-adrenal system that governs cortisol release, is designed for acute activation with complete recovery. Cortisol spikes in response to threat, mobilizes resources, and then is cleared as the parasympathetic system restores baseline. This cycle can run thousands of times across a lifetime without structural consequence, provided the recovery phase completes each time.
The problem arises when recovery is chronically incomplete. When the next demand arrives before cortisol has returned to baseline, the system begins operating from an elevated set point. The hippocampus (dense with glucocorticoid receptors and essential for contextual memory, emotional regulation, and stress modulation) undergoes dendritic retraction under sustained cortisol exposure. Hippocampal volume reductions of 5-12% have been documented in individuals with chronic stress exposure. The prefrontal cortex loses dendritic branching and synaptic density under the same chronic stress, acting mainly through excessive catecholamine signaling. The amygdala, by contrast, shows dendritic growth under chronic stress, becoming more reactive precisely when the structures that regulate it are becoming less capable.
This is the neuroanatomy of the breaking point. Not a metaphor. Not a moral failure. A measurable erosion of the brain’s regulatory architecture driven by chronic stress overload, and a process that can be reversed when the right conditions for neural recovery are established.
Why Some People Recover Faster: Vagal Tone and mPFC Regulation Capacity
One of the most persistent questions in resilience neuroscience is individual variation: why do some people recover from identical adversity in days while others remain destabilized for months? The answer is not psychological toughness. It is physiological, rooted in two measurable systems that differ substantially across individuals.
The first is vagal tone: the tonic activity level of the vagus nerve, the primary parasympathetic pathway connecting the brainstem to the heart, lungs, and visceral organs. Stephen Porges’ polyvagal theory and subsequent research have established that individuals with higher resting vagal tone show faster physiological recovery from stress, greater flexibility in autonomic regulation, and more efficient return to baseline after emotional activation. Vagal tone is typically measured through heart rate variability, the beat-to-beat variation in cardiac rhythm, which reflects the vagus nerve’s moment-to-moment modulation of heart rate.
High vagal tone is not simply the absence of stress reactivity. It is the capacity for rapid state transitions: moving from high arousal back to calm efficiently, without residual physiological activation. Individuals with high vagal tone can mount a full stress response when needed and then clear it when the demand resolves. Those with low vagal tone remain in physiological activation states long after the triggering event has passed, which is why a single difficult conversation on Monday morning can produce elevated cortisol, disrupted sleep, and impaired cognitive function through Wednesday.
The second system is mPFC regulation capacity: the medial prefrontal cortex’s ability to generate inhibitory signals strong enough and fast enough to modulate amygdala activation. This capacity is not fixed. It varies with sleep quality, stress and nervous system regulation history, prior adversity exposure, and, most importantly, the degree to which the mPFC has been specifically engaged in regulatory learning. The brain strengthens the circuits it uses. An mPFC that has been systematically trained to regulate emotional responses under real conditions builds denser connectivity to the amygdala, faster signaling speed, and more robust inhibitory output.
The Myth of Mental Toughness as Willpower
The popular concept of mental toughness implies that resilience is fundamentally an act of will: that resilient individuals simply choose to push through, refuse to quit, and muscle past adversity through sheer determination. This framing is neurologically inaccurate, and worse, it is counterproductive. It leads people to rely on the exact cognitive strategy that fails under the conditions where resilience is most needed.
Willpower is a prefrontal cortex function. It depends on dorsolateral prefrontal activation, which requires glucose, adequate sleep, and low competing cognitive demands. Every act of effortful self-regulation depletes these resources. Roy Baumeister’s ego depletion research, despite ongoing methodological debate, identified a real phenomenon at the neural level: prefrontal regulatory capacity is finite within any given period, and it degrades under sustained demand.
This means that willpower-based resilience fails precisely when it is needed most: during high-stress, high-demand periods when the prefrontal cortex is already running at diminished capacity. The individual who has been suppressing emotional responses, maintaining composure in back-to-back high-stakes meetings, and effortfully controlling their behavior all day has progressively less prefrontal resource available for the next demand. The eventual failure is not weakness. It is resource depletion in a system that was never designed to sustain effortful control indefinitely.
Genuine resilience does not depend on willpower. It depends on automaticity: neural patterns that regulate emotional responses without requiring conscious effort or prefrontal expenditure. When the prefrontal-amygdala regulatory pathway is well-conditioned, emotional modulation happens at the circuit level, below conscious awareness, at speeds that precede voluntary control. The resilient individual does not decide to remain calm. Their regulatory architecture produces calm as a default output because the circuit has been trained to generate that response automatically.
This distinction between effortful regulation and automatic regulation is the difference between resilience that looks impressive for a week and resilience that operates under genuine duress for years.
HPA Axis Flexibility vs. Rigidity: The Signature of Resilient Neurobiology
The HPA axis is not a switch. It is a dynamic system capable of extraordinary nuance, but only when it retains its flexibility. The distinction between a flexible HPA axis and a rigid one is one of the most consequential findings in resilience neuroscience, and it maps directly onto clinical observations about who thrives under pressure and who fragments.
A flexible HPA axis responds proportionally to demand. Minor stressors produce minor cortisol elevations. Major stressors produce appropriately large responses. And critically, the system returns to baseline rapidly when the demand resolves. The cortisol curve is steep on the way up, proportionate in magnitude, and steep on the way down. This flexibility is governed by an intact negative feedback loop: glucocorticoid receptors in the hippocampus and prefrontal cortex detect rising cortisol and signal the hypothalamus to reduce further output.
A rigid HPA axis has lost this proportionality. It may produce blunted cortisol responses to genuine threats, failing to mobilize adequate resources, or it may produce exaggerated responses to minor stressors, flooding the system with cortisol for situations that warrant only modest activation. The cortisol awakening response, which should show a sharp spike within 30 minutes of waking followed by a gradual decline, becomes flattened or dysregulated. The diurnal rhythm (high morning cortisol, low evening cortisol) loses its shape.
HPA axis rigidity is both a consequence and a cause of reduced emotional resilience. Chronic stress produces rigidity. Rigidity amplifies vulnerability to subsequent stress. The loop perpetuates. But the neuroscience is equally clear that this rigidity is reversible. The glucocorticoid receptor density in the hippocampus can increase. The negative feedback loop can be restored. The diurnal cortisol rhythm can be recalibrated. The HPA axis, like every other neural system, adapts to the demands placed on it, and when those demands include systematic resilience-building conditions, the system rebuilds its flexibility.
Post-Traumatic Growth: Neuroplastic Reorganization After Adversity
Resilience neuroscience has moved beyond the question of recovery, returning to a previous baseline, and into a more provocative territory: post-traumatic growth, the documented phenomenon in which individuals not only recover from adversity but emerge with capacities, perspectives, and neural resources they did not possess before the disruption.
The neuroscience of post-traumatic growth is rooted in neuroplasticity: the brain’s capacity to reorganize its structure and function in response to experience. Adversity, when it does not exceed the system’s capacity to process it, creates conditions of intense neural activation that are also conditions of intense plasticity. The same elevated metabolic state that makes stress damaging under chronic exposure makes it a powerful catalyst for reorganization under controlled conditions.
Neuroimaging research has documented structural changes associated with post-traumatic growth: increased prefrontal cortical thickness, expanded white matter connectivity between regulatory and emotional processing regions, and enhanced default mode network integration: the brain network associated with self-reflection, meaning-making, and future planning. These are not metaphorical changes. They are measurable structural adaptations that produce genuinely new cognitive and emotional capacities.
The critical variable is not whether adversity occurs, it will, but whether the brain has the architectural support to process the experience through reorganization rather than through defensive rigidity. An mPFC with strong connectivity to the amygdala, an HPA axis with preserved flexibility, a vagal system capable of efficient state transitions: these are the conditions under which adversity produces growth rather than damage. This is why resilience architecture matters before the crisis arrives. The brain that enters adversity with robust regulatory infrastructure is the brain most likely to exit it transformed rather than diminished.
Building Resilience at the Circuit Level
In my practice, I approach emotional resilience the way a neuroscientist approaches architecture, not as a quality to be admired or a trait to be wished for, but as a neural system that can be assessed, mapped, and deliberately strengthened at the circuit level. The distinction between this approach and conventional resilience work is not philosophical. It is methodological. And it determines whether the results are temporary or durable.
The first principle is specificity. Resilience is not a single capacity. The prefrontal-amygdala pathway governs emotional regulation under acute stress. The vagal brake governs physiological recovery speed. The HPA axis flexibility determines proportionality of cortisol response. The default mode network integration shapes meaning-making capacity after adversity. Each of these systems can be independently assessed and independently trained. A program that treats resilience as a monolithic quality misses the architecture, and an intervention that misses the architecture produces motivational results without neurological change.
The second principle is state-dependent learning. Neural circuits are most plastic when they are active. The prefrontal-amygdala pathway is most available for strengthening during moments when it is actually engaged in regulation, not during calm reflection about past stressors, but during live encounters with the neural activation patterns that challenge the system. Real-Time Neuroplasticity™ operates within these high-plasticity windows because the neuroscience is unambiguous: the conditions under which a circuit was built are the conditions under which it is most efficiently rebuilt.
The third principle is that resilience is not the absence of reactivity. It is the quality of recovery. The goal is not a brain that fails to register threat: that would be pathological. The goal is a brain that registers threat accurately, mounts a proportionate response, and clears the activation efficiently, preserving regulatory resources for the next demand. Every element of this (cortisol and adaptive stress response calibration, vagal recovery speed, prefrontal regulatory output) is trainable through precise, individualized work at the neural architecture level.
The individuals I work with are not fragile. They are operating with regulatory systems that have been shaped by decades of demand without adequate recalibration: systems running patterns that were adaptive in earlier environments but are now producing disproportionate responses to current conditions. The architecture can be restructured. The connectivity can be rebuilt. The flexibility can be restored. What is required is work that matches the precision of the neuroscience to the specificity of the individual brain producing the pattern.
If your capacity to recover from setbacks, regulate under pressure, or maintain clarity during sustained difficulty is costing you in the areas that matter most: schedule a strategy call with Dr. Ceruto. I will assess your specific resilience architecture and identify where the circuit-level recalibration needs to occur.